02 Nov THE BUTTONHOLE TECHNIQUE
Edited by Marisa Pegoraro
In our Hospitals and Dialysis Centres there is a growing tendency to use the so-called Buttonhole technique, also and above all for those who choose home dialysis. It is important to understand what it consists of, when it can be used and how to maintain its fistula. Marisa Pegoraro talks about it below.
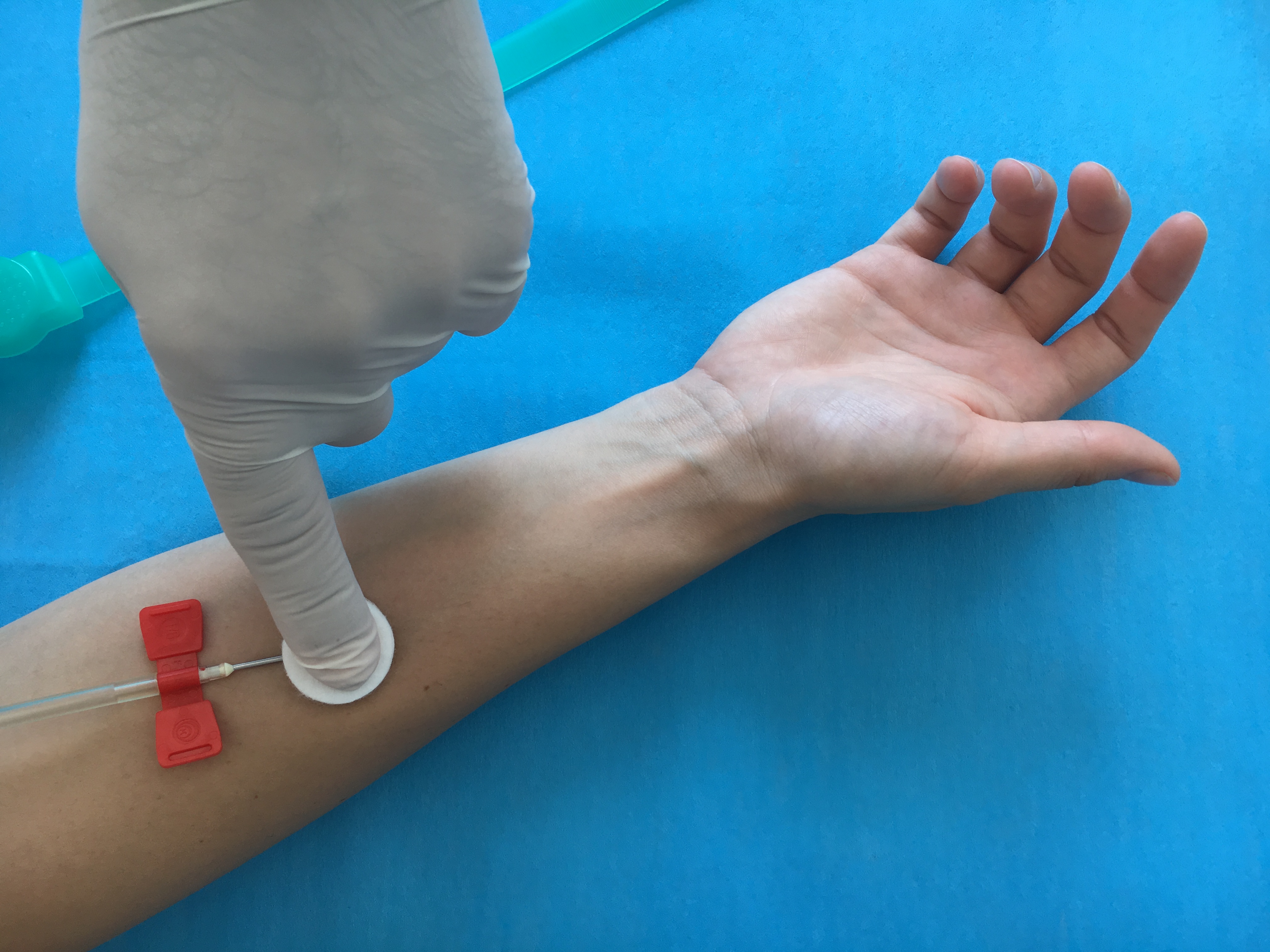
The Buttonhole technique – literally an eyelet, buttonhole – requires the needles to be placed in exactly the same point and with the same inclination and position for each dialysis session. Before inserting the needles, the area must be washed, disinfected and the scabs removed following a simple management protocol that MUST always be followed. If possible, the needle insertion sites are chosen together with the patient. They must be linear areas, not located at joints or in particularly painful points, to allow the patient to insert the needle himself. After making a number of punctures with the usual sharp needles – at least 6 – it is possible to use needles that appear to be the same as the previous ones but which do not have a cutting edge, they are pointed, but not sharp and the tips are blunt. These are needles that can only be used where a scar “pathway” has already been created, where there is reduced tissue cohesion. The blunt needle moves the fibres apart and always reaches exactly the same point of the vein, where a breach is created that can be easily penetrated by the needle. It is very important to insert the needles properly and delicately. This allows them to follow the “pathway” that was already created by the other needles.
WHEN TO CHOOSE THE BUTTONHOLE TECHNIQUE: CLINICAL CHARACTERISTICS OF THE PATIENT
Theoretically, the Buttonhole technique can be used for all patients; however, because it involves special hygiene and practical skills, it also requires two essential components: motivated and competent nurses and focused and cooperative patients. For people with immune system diseases or chronic diseases that make them more vulnerable, or for those who are unable to carry out arm hygiene on their own, the Buttonhole technique may not be the right choice. The risks associated with this technique, if not well performed, may outweigh the benefits and this leads healthcare professionals, doctors and nurses to prefer other puncture techniques.
ADVANTAGES OF THE BUTTONHOLE TECHNIQUE:
- Ugly bulges, referred to as aneurysms, do not form because when you always puncture at the same point the vein wall remains solid and don’t deform.
- Less pain. Even if it is very subjective, the pain experienced is on average less than it would be if you always punctured different sites, because the sensitivity decreases as the “pathway” is structured. This is especially useful for those with a low pain threshold or those who are afraid of needles (agophobia) and in paediatric and youth dialysis.
- Reduces puncture errors. Errors when puncturing can cause bruising and extravasation of blood around the vein. This not only concerns the patient, but also the nurse who in this way potentially causes less damage and less pain.
- Shorter haemostasis time at the end of dialysis, even in subjects undergoing OAT treatment (Oral Anticoagulant Therapy), because the healthy elastic skin around the sites allows it to heal quickly.
DISADVANTAGES OF THE BUTTONHOLE TECHNIQUE:
The only major drawback of the Buttonhole, patients are more susceptible to infections. Experience in recent years confirms that infections can occur only if the procedures are not properly applied. Another frequent but less important factor that involves some nurses and patients is the attachment time. This increases by about 5-10 min in order to apply the protocol correctly, removing of the scab and inserting the blunt needle, which is a gentler but slower procedure compared to using a sharp needle. A crucial aspect is the training of nursing staff regarding compliance with the dialysis protocol and the use of the blunt needle.
INFECTION OF THE BUTTONHOLE FISTULA: HOW IS IT TREATED AND MORE IMPORTANTLY HOW IS IT PREVENTED?
Infection of the fistula is the critical point of the Buttonhole technique. Studies conducted on this subject have shown that, if the arm washing protocol is strictly applied just before dialysis, followed by the thorough “disinfect-remove scab-disinfect” (d-r-d) procedure, the chances of infection become extremely remote. This problem can be eliminated completely if we add post dialysis care and, if necessary, use specific dressings.
HOW TO MEDICATE A BUTTONHOLE FISTULA IN HOSPITAL AND AT HOME
At the end of the dialysis, and after haemostasis, remove any residues of blood using a physiological solution and apply the dressing. The dressing should be kept for at least 5/6 hours after the end of dialysis. If you suffer from skin disorders, for example psoriasis or autoimmune diseases such as lupus, or, if for some reason you notice redness around the exit-site, it is advisable and recommended that you apply “advanced” dressings (e.g. silver) before the top dressing. Silver should not be used together with disinfectant due to its naturally antibacterial and healing action.